Femoroacetabular Impingement (FAI) and Hip Pain
By: Dr. Kevin McIntyre B.Kin., DC
Hip pain is common. There are many different causes for hip pain, and the diagnosis depends on many different factors. These factors include age, mechanism of pain, pain location and aggravating factors, to name a few. Perhaps one of the most common causes of painful hips in elderly patients is osteoarthritis. Osteoarthritis is degeneration of the joint surface. It isn’t always painful, and most of us walk around with a normal amount of pain-free wear and tear in our joints. In severe cases of degeneration, it can become painful and make walking difficult. Unfortunately, for those patients who don’t respond to conservative measures, hip replacement is often required. Thankfully, these procedures have become quite common, and a favourable outcome is somewhat likely.
Degenerative arthritis and hip replacement are not common for younger patients. In younger patients, we can often attribute their hip pain to a muscular injury in the area or a temporary irritation of a bursa. These are not long-term structural injuries. Unfortunately, conditions related to the actual hip joint may be considered more of a structural condition and may have a more complicated recovery path. These diagnoses include (but are not limited to) femoroacetabular impingement (FAI), acetabular dysplasia or cartilage/labral injury.
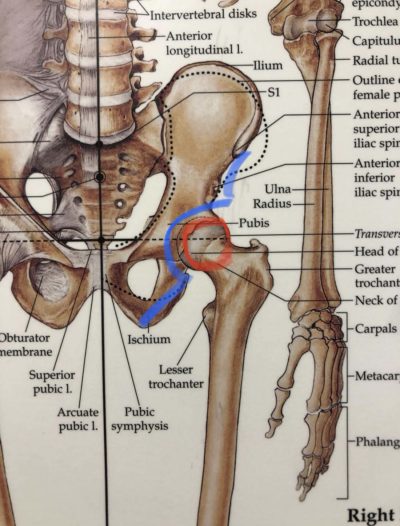
The hip joint can be described as a “ball and socket” joint and is perhaps the easiest way to visualize some of these structural changes that can occur. The “ball” is outlined in red below, and the “socket” on the pelvis is outlined in blue.
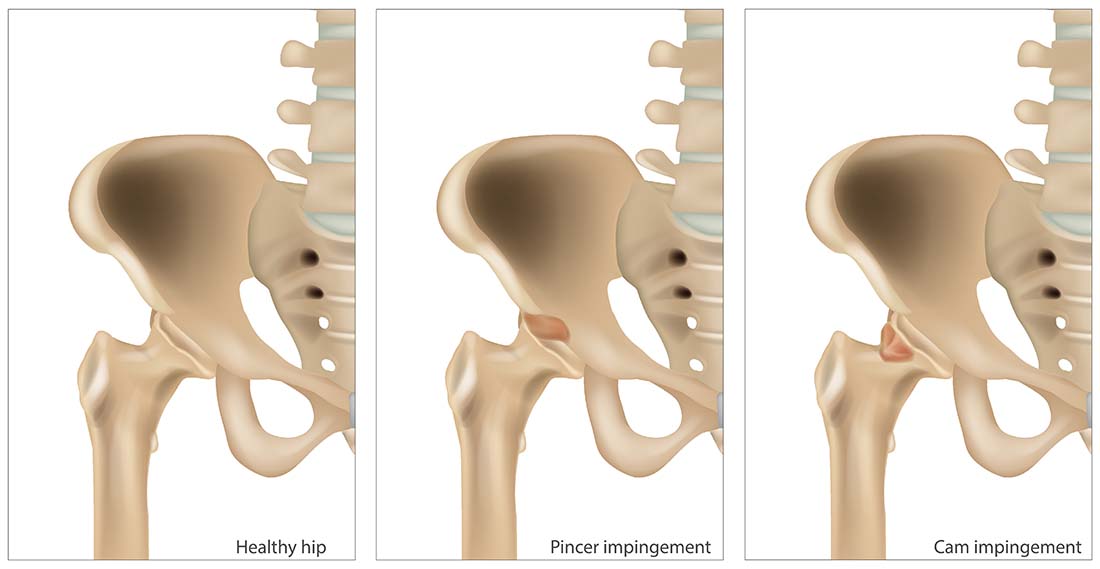
Femoroacetabular Impingement
Femoroacetabular impingement occurs when the shape of the ball or the socket in the hip joint isn’t quite perfect. There are two primary types. A “cam” type is when the ball of the hip joint isn’t quite a round surface and butts into the pelvis (the socket). A “pincer” deformity is when the socket surrounds the femoral head (the ball) and creates impingement of the structure as it moves. Both deformities are visible on x-ray or MRI, but these tests aren’t always necessary.
There are clinical tests we can also utilize to try and identify hip injuries. These tests are a combination of movements to challenge the area; flexion/adduction/internal rotation (FADIR), flexion/internal rotation (FI-R), flexion/abduction/external rotation (FABER) and also internal rotation in a neutral hip position. An interesting study that was published in The British Journal of Sports Medicine found that the restricted internal hip rotation in neutral hip flexion (with the knee bent while the patient is lying on their stomach) was the best test to rule in FAI and a lack of pain with the FADIR test and a lack of restricted motion with the FABER test were best to rule out FAI. This may be a little bit technical for our average reader, so the take-home point is that we can use some tests in the clinic to help figure out the nature of your pain!
Treatment for Hip Pain
The treatment for hip pain is very specific to the individual and their specific case. As for most musculoskeletal conditions, strengthening and home exercise is a prudent strategy with good supporting evidence. The frequency, intensity and type of exercise will be quite variable, so some professional guidance is recommended. For example, plyometric exercises might be appropriate for an active person returning to sport, while some people might see a rather significant irritation of symptoms with relatively simple exercises. Although there is good supporting evidence for surgery (which is somewhat surprising), we usually recommend conservative care as a first consideration. Conservative care includes strength exercises, stretching and clinical treatment like active release, graston, acupuncture and laser.
In summary, there are many different causes of hip pain, and the treatment is variable. There are some cases that require a more experienced diagnostician to help identify the cause of pain, and some clinical tests have good supporting evidence for their use. There is always something we can offer to help our patients with hip pain. Although surgery is indicated in rare occasions, most cases improve with a little guidance from a professional.
References
Ishoi L, Nielsen MF, Krommes K, Husted RS, Holmich P, Pedersen LL & Thorborg K. Femoroacetabular impingement syndrome and labral injuries: grading the evidence on diagnosis and non-operative treatment – a statement paper commissioned by the Danish Society of Sports Physical Therapy (DSSF). British Journal of Sports Medicine 2021; 55: 1301–1310. doi:10.1136/bjsports-2021-104060.
Reiman MP, Agricola R, Kemp JL. Consensus recommendations on the classification, definition and diagnostic criteria of hip-related pain in young and middle-aged active adults from the International Hip-related pain research network, Zurich 2018. Br J Sports Med (Published Online First: 20 January 2020).





